

What the Last Half Century Has Done for a Congenital Upper-Limb Amputee

WORDS Melissa Bean
I used to traverse the monkey bars during elementary school recess using the crook of my left elbow and right hand. My callouses were magnificent. I’m an upper-limb, below-elbow congenital amputee. As hard as it was to figure out how to swing like a monkey with only one hand, the worst part was taking off my prosthesis at recess.
I had to—it wrecked my rhythm. The moment the bell rang, I would rush out to the bars, pull off my harness, unsnap the straps, yank my arm out of the socket and roll down the liner—usually one of my own socks. By the time I dropped my prosthesis onto the ground in a tangle, there would be a crowd of curious first, second, and third graders standing around me.
I got my first prosthesis in 1975 when I was 18 months old as part of a beta test of my age group for the Child Amputee Prosthetics Program (CAPP). I have whisper-thin memories of my time in CAPP, but all of them are happy. I stayed with the program, at its University of California Los Angeles (UCLA) hub, until I was eight. That’s when, right on the school playground, I broke the cable of my body-powered prosthesis. When my parents asked if we should go to UCLA to have it repaired, I said, “No thanks.”
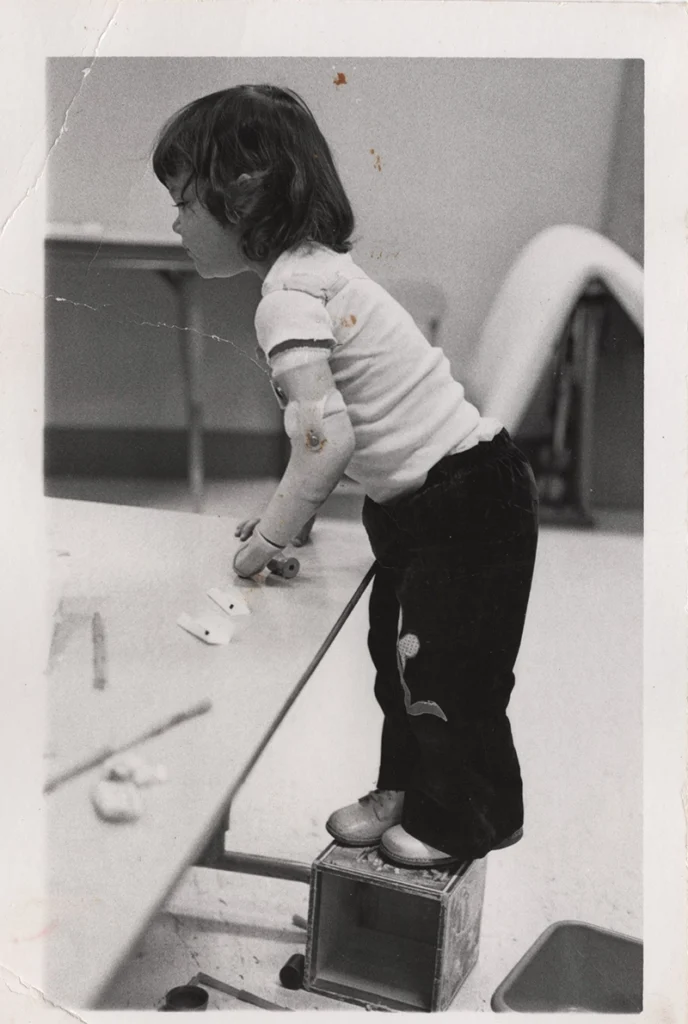
By the time I was in third grade, I had a body-powered arm modeled on my unaffected limb. But on the swings, in the jungle gym, and under a jump rope, my “helper” didn’t feel helpful. It was heavy, rock hard, and frozen at an obtuse angle. My prosthesis was intended to be lifelike, but from my point of view it was a cosmetic device meant to make me look like everyone else, while preventing me from feeling capable.
Even though I stopped using a prosthesis, CAPP taught me how to be a one-handed person more than any other individual or entity. The doctors, prosthetists, and therapists modeled the kindness, acceptance, creativity, and determination I would need to succeed in a two-handed world. Even as they focused on my limb difference, teaching me to use my hand and my prosthesis effectively, they treated me like a typical kid. They showed me how to balance being special but also ordinary.
At age 53, the overuse injuries all amputees experience have caused me to reconsider prosthetics and my disability, leading me to obtain a soft-socket, passive Koalaa I use for specific tasks. And I’ve joined online groups for congenital amputees and attended gatherings for amputees in Southern California. Most recently, I was a patient model for orthotics and prosthetics (O&P) master’s degree students at California State University Dominguez Hills (CSUDH).
That’s where all my impressions from wearing a prosthesis as a child and all my questions about using a prosthesis as an adult collided.
Serving the Child Amputee
On my first afternoon as a patient model at CSUDH, I sat for two castings. There wasn’t time to finish my socket that day, so I tried out a myoelectric hand/wrist simulator that bore quite a resemblance to the disembodied hand, Thing, from The Addams Family. Besides students, faculty, patient models, and heavy equipment, the CSUDH workshop was an interactive exhibit of prosthetic arms, legs, feet, and hands in every stage of fabrication—like a garage sale of body parts. With a small crowd of single-minded and enthusiastic O&P students around me, I synced up my thoughts with Thing and managed to turn the hand at the wrist and make the thumb and index finger open and close. There were cheers. I felt like a genius. I felt like I had saved the princess in Super Mario Brothers. I didn’t feel like I’d grown a limb, but my cheeks hurt from smiling, and I didn’t want to stop.
Faculty Instructor Steven H. Alpert found out I grew up in Southern California and immediately asked, “Were you in CAPP?”
The engineering department at UCLA started its Research Program in Upper Extremity Prosthetics in 1946, and CAPP was a secondary development in 1953. Not long after, the program received a grant from the United States Children’s Bureau.
“This is during a period of time where we were federally funded, and there was a lot of research going on. The biggest change that occurred over the decades is that initially we didn’t have a lot of component options for children. They were not small enough,” Alpert says. “We got the CAPP terminal hand, the Sentry hand, and the chest harness.”
When I started in the CAPP in the 70s, it was evident thalidomide would not have much impact in the United States, but its threat had driven huge prosthetic advances in devices for children. One, the CAPP terminal device, is the first I remember using. Alpert joined the staff of CAPP in 1988 and helped transition the program from UCLA to Shriners Hospitals for Children.
Alpert is a dedicated advocate for one of CAPP’s enduring developments.
“The whole premise of CAPP was a multidisciplinary team approach. This is the model I believe in and what I worked with in multiple institutions where you had a physician, surgeon, social worker, occupational therapist, physical therapist, and prosthetist. Each discipline evaluated the patient, and collectively we would come up with a protocol for fitting the patient,” Alpert says. “I always tell my students, if you don’t work in a multidisciplinary approach you need to create it.”
Choosing a Giving Profession
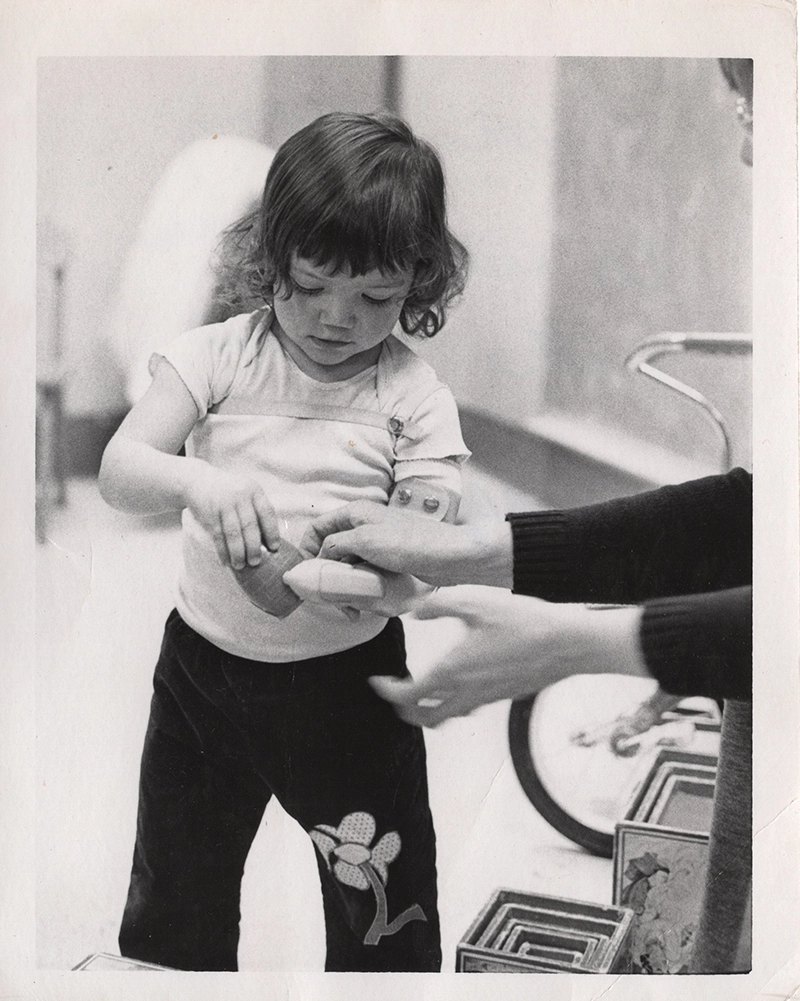
Alpert mentioned a few names from CAPP, but I only remember one person from my CAPP days, my occupational therapist, Cass. Cass was just about my favorite person in the world, right up there with my best friend Allison and my Nana. Twice a week, my mom, Nana, and I made the hour-and-15-minute drive to the clinic—an errand usually punctuated by a lunch of chili cheese spaghetti at Bob’s Big Boy. I don’t know how my mother and grandmother felt about the commute, but no one had to force me into the car. I was going to see “my Cass.” I adored her.
Cass was lovely and patient, always smiling, and had dark brown hair like mine. We were going to put on my “helper” and play with toys, blocks, and cute dolls who always needed their shoes tied, dresses zipped, and jackets buttoned. I enjoyed the attention and was too young to know I was having a singular experience. Meeting the master’s degree students at Dominguez Hills showed me there is a consistent theme among people who work with amputees—these are people who care.
A soccer injury led Olivia Beamish to seek a master’s degree in O&P. After surgery on her knee, she had a life-changing experience in physical therapy. “They were so encouraging. They said, ‘We will get you back to playing.’ They gave me a part of my life back that I thought was gone,” Beamish said. “I started thinking about people who lose limbs and wondered who helps those people? Losing a limb is more serious than tearing a ligament. So I started researching, and I decided that’s what I wanted to do.”
Beamish has always loved building and problem-solving, so she had planned to study engineering. Her education in O&P began with an undergraduate degree in biomedical engineering at California State University Long Beach. She sees the future of the profession as a combination of technology and the foundations of prosthetics.
Mark Cromer, CSUDH faculty instructor, says the focus on the patient and the craft need to stay at the forefront of prosthetics education.
“It’s important that we understand what we were doing and why we do it. As an industry, we have been losing the emphasis on being craftsmen and on building a prosthetic as a labor of love. Sometimes the focus ends up on saying the right words, patients per day, billing, and getting reimbursed,” he says. “The emphasis on technology is particularly marketed. It’s a great tool, and for sure we can do things that we couldn’t do before, but it’s more about how you apply the tool than the tool itself.”
Redefining Amputation
The wider world sees prosthetics as an offshoot of science fiction.
“There is a fantasy about the tech that it will give us the Star Wars-like arm or the ability to run faster and jump higher. That’s a possibility, but the timeline is much further out than people want to believe. We have to struggle through these awkward stages to get to the state of the art, and I think we’re doing pretty well for the size and scope of our profession,” Cromer says. “There are obstacles. There is a large profit motive in the industry that drives trends but is not necessarily the best long-term plan. I tend to see people getting stuck on that vision and not giving the attention to the fundamentals.”
Cromer is a lower-limb amputee with a left rotationplasty and knows firsthand about the high stakes. “For upper extremities, 40 to 80 percent of prosthetics are not used. The more proximal the level, the higher the rejection. We combine a teaching approach with full facilities to teach clinicians to fit a prosthetic that will be useful and used, because if it doesn’t fit it hurts and now it’s thrown in the closet,” he says.
At age 50, with adult-onset scoliosis and chronic De Quervain tenosynovitis causing me constant pain and limiting my activities, I spoke to my general practitioner about getting a prosthesis. I was casted and tried two test sockets at a clinic in my city. However, the model the prosthetists chose was heavy and the fit of the socket hurt so much I had to do a little Lamaze breathing. What frustrated me the most about the experience was the same frustration I felt as a child—I didn’t want or need a prosthesis to replace a hand I have never had.
Adding length to my residual limb would ease my back pain, and components that could stabilize objects while I manipulate them would improve my tenosynovitis. The clinicians I worked with truly attempted to build a prosthesis that would work for me, but they did not comprehend the differences between my needs as a congenital amputee and the needs of the acquired amputees they had been trained to treat.
“For a patient with an acquired limb loss, they really want to be able to feel like their normal previous self. Congenital amputees have learned to live with their limb difference to the point where they may not need a device or might feel like a prosthetic interferes with their abilities,” says Victoria Holt, a CSUDH master’s degree graduate.
Holt did her undergraduate work in kinesiology at California State University San Bernardino. After completing her master’s degree at CSUDH in May, she began a residency at O&P company Lerman and Son. Upper-limb prosthetics are her main interest, and she plans to study the different needs of acquired and congenital amputees.
“We worked with a congenital amputee patient model who said she would rather live with overuse injuries than wear a prosthetic, because in her mind, she would be losing the connection to her environment and that is more important than anything.”
Returning to Prosthetics as a Craft
During the 1980s, funding for child amputee programs began to disappear. Research ended, many O&P schools closed, and the industry went into survival mode. The history of the prosthetics program at CSUDH through the 90s and early aughts is a chaotic but determined tale of competing for grants, struggling to find facilities, and scraping to pay for materials, all while trying to train future clinicians and meet the new standards of prosthetics education. Students were taught in off-campus warehouses and missed out on vital aspects of campus life, including general coursework and health insurance.
In 2014, the minimum education level for a practicing prosthetist was raised to a Master of Science degree, and CSUDH traded its bachelor’s and certificate programs for a master’s program. Clinicians are also required to accomplish an 18-month residency after they earn their degrees and then sit for board exams to become nationally certified. There are 15 universities in the nation with accredited master’s degree programs in O&P.
Mark Muller, O&P department chair at CSUDH, has many responsibilities, including tracking down every resource he can find and, with only logistical support from the university system, gathering the funds and loans necessary to keep the program operating and building its new facilities. Faculty, students, and staff moved into a state-of-the art lab in January. It has equipment and space for plastics, plaster, machining, fabrication, and CAD, as well as classrooms, lecture rooms, and outdoor workspace.
“We are the only program in the California university system paying its way to be here. I have to manage my own budget for custodians, electricity, patient models, plastic, plaster, and all of the pieces and parts that go into a business in an educational setting,” he says. “Now we are trying to find more ways to add value without increasing tuition.”
Muller is bringing new programs to the university, including an assistant mastectomy fitter program, a technician program, and a veterinary O&P program. CSUDH has also partnered with Angel City Sports, a nonprofit that provides adaptive sports opportunities, and the group will be moving its headquarters to CSUDH’s facility on campus. The university also houses and staffs the Ottobock Repair Center for the 2028 Paralympic games. CSUDH’s O&P program has 15 alumni Paralympians and 100 alumni Paralympic coaches.
“We make a really good return on investment for our students—100 percent of them end up with a lucrative career where they only help people, and do not hurt anyone. This is a serving profession, not a taking profession,” Muller says. “And we know what our job is. We are to make our students competent practitioners—and not just in theory.”
An essential part to the success of CSUDH students is interacting with amputees themselves. With 30 students on the practitioner level, the program needs 15 models each for its upper-limb, lower-limb, and spinal projects.
A New Kind of Arm
I will show up any time CSUDH calls me. There are very few scenarios in the life of an amputee where having a limb difference is considered an asset and is met with genuine, productive enthusiasm. Besides that, I learned a powerful lesson about my future as a congenital amputee.
I have never thought a prosthesis could really work like a hand. I use my Koalaa for specific tasks, and it is an effective and practical tool. It took me a while to stop feeling like I was going to hit myself in the face with my extra-long arm, but I got used to it. Also the Koalaa is highly adjustable, so I cut off an inch, and that did the trick. However, experimenting with the myoelectric hand at CSUDH blew my mind. For one, it didn’t hurt—Beamish and several other students worked on my test socket for hours.
The system for setting and calibrating the sensors was completely fascinating. I could see the uptick in electrical activity on the screen before I even recognized I was thinking about moving the test hand fingers. While the students watched the feedback on the monitor discussing “pattern recognition” and “gains,” I was watching the indicators move up and down exclaiming, “Is that me? Is that me?!” It felt less like a video game and more like the possibility of a truly helpful working prosthesis.
I spent so many years pushing myself to live and function as a two-handed person, it is still an effort to remember I do have limitations, and I am allowed to take support when it’s offered. I’d been given the impression that my age and the many years I’d lived without a prosthesis meant I did not have the neural pathways necessary to use a myoelectric prosthesis. Finding out otherwise has been life-altering.
I went into the patient model project thinking only about what I had to offer the students in the program with no idea I might learn something extraordinary. I thought I knew everything about living as a congenital amputee. Then I saw five fingers on the end of my residual limb moving the way I asked them to move, and it has given me an entirely new way to consider prosthetics and how they might work in my life.
Child Amputees
Orthopedic surgeon Dr. Charles H. Frantz (1906-1978), the first chairman of the Subcommittee on Child Prosthetics Problems for the National Academy of Sciences Committee on Prosthetics Research and Development, had a major role in identifying not just the need to serve child amputees, but also discovering their actual numbers and bringing them to the forefront of the field of prosthetics.
Frantz stated in 1966 in a report written on the evolution of care of the child amputee that “prior to World War II, no precise methods of management existed. Common practice in fitting a child amputee with a prosthesis involved procrastination.”
1946: An amputee training center was opened at the Mary Free Bed Guild Children’s Hospital and Orthopedic Center in Grand Rapids, Michigan.
1950: Professionals from the training center studied 192 cases of child amputees and produced a 28-minute movie illustrating the problems of the child amputee and demonstrating techniques for fitting and training. “Thus,” Frantz wrote, “for the first time, the child amputee was identified as an entity to the medical community.”
1956: There were four prosthetics clinics in the United States that specialized in treating children. Clinicians had begun the development of child-sized prosthetic components.
1966: There were 20 prosthetics clinics in the United States that specialized in treating children. Frantz wrote that early statistics showed “a ratio of two post-traumatic or post-surgical amputees to one congenital amputee.” Most likely due to the publicity about the treatment program, children came to clinics at younger ages and greater numbers. The ratio changed to five children with congenital amputations for every two with acquired amputations.


