Earlier this year, the American Heart Association threw its weight behind a campaign to drastically reduce limb loss related to diabetes and peripheral artery disease (PAD). Those two conditions cause slightly more than half of all U.S. amputations, or an estimated 100,000 amputations a year. The AHA’s goal is to reduce limb loss by 20 percent before the end of this decade—that’s about 20,000 prevented amputations every year, a rather large impact.

To help set a baseline for that initiative, the AHA released a followup study last month documenting rates of vascular-related amputations across a range of demographic categories. Published in the Journal of the American Heart Association, the paper analyzes how frequently vascular disease leads to amputation within disparate geographic regions, racial and ethnic populations, income categories, and so forth. Because it examines a huge population—nearly 200,000 Medicare-eligible patients who lost a limb to diabetes or PAD between 2010 and 2018—the paper gives us a pretty detailed picture of the most vulnerable populations.
The JAHA paper goes out of its way to distinguish between total amputation numbers and amputation rates per capita. Total numbers, not surprisingly, are highest in urban centers with large populations: about 150,000 of the amputees in the study live in metropolitan zip codes, nearly four times the number who live in rural zip codes. Likewise, a majority of the patients are Caucasian, broadly reflecting the nation’s overall racial profile.
However, amputation rates tell a much different story, illuminating key gaps in the current health-care system—and key opportunities to reduce future limb loss.
One major finding: rural Americans face an elevated risk of limb loss related to PAD and diabetes. The JAHA study assigned every zip code in the US to one of three categories: metropolitan, rural, or micropolitan. (The latter refers to small cities of 10,000 to 50,000 residents.) Per capita, limb loss was about 15 percent more common in rural zip codes than in urban ones, an outcome the study’s authors attribute to the relative scarcity of health care services in rural communities.
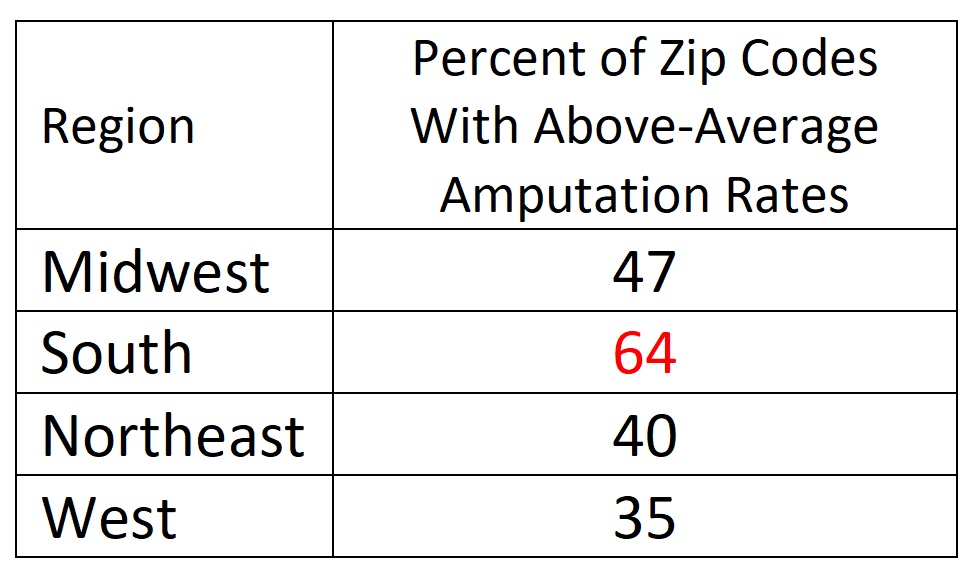
Another conclusion, echoing the outcomes of previous studies, is that the South has a disproportionately high incidence of limb loss due to diabetes or vascular disease. The JAHA study divided the country into four regions (Northeast, South, Midwest, and West), then sorted zip codes by amputation rates. Almost half of all zip codes with above-average rates of limb loss are located in the South.
This parsing is slightly misleading, because the number of zip codes is not equal across regions—the Midwest and South have more zip codes than the Northeast and West. Even taking that into account, however, the South harbors an inordinate share of communities with high amputation rates. In nearly two-thirds of the zip codes in the South region, amputation rates exceed the national average. That’s by far the highest prevalence in the nation:

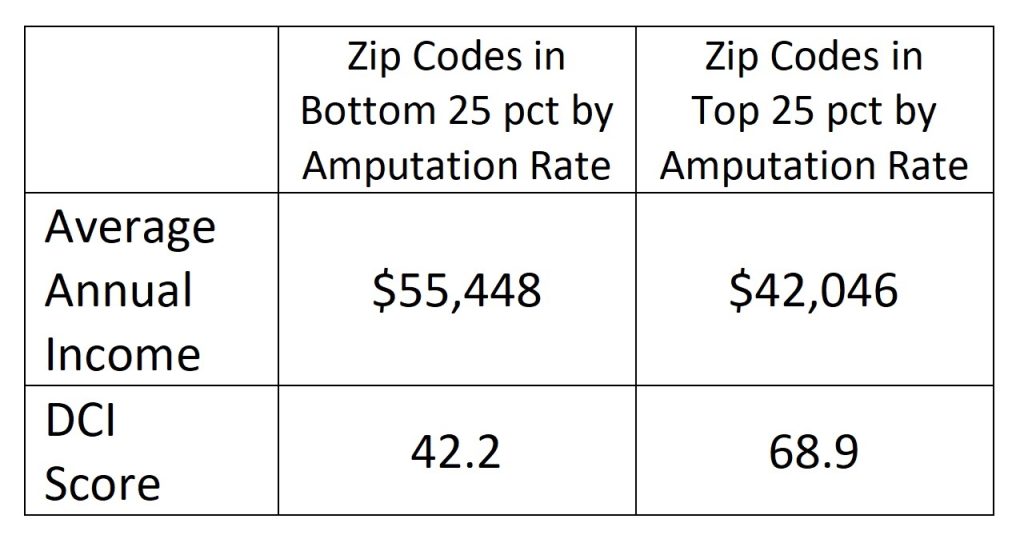
Income is a third major factor affecting the frequency of limb loss due to PAD/diabetes. According to the JAHA study, households in zip codes with the lowest amputation rates earned about 33 percent more, on average, than households in zip codes with the highest amputation rates. Likewise, low-amputation zip codes had much lower scores on the Distressed Communities Index (DCI) than high-amputation zip codes. (The DCI integrates factors related to income, education, employment, and business activity; higher scores correlate to higher economic instability.)

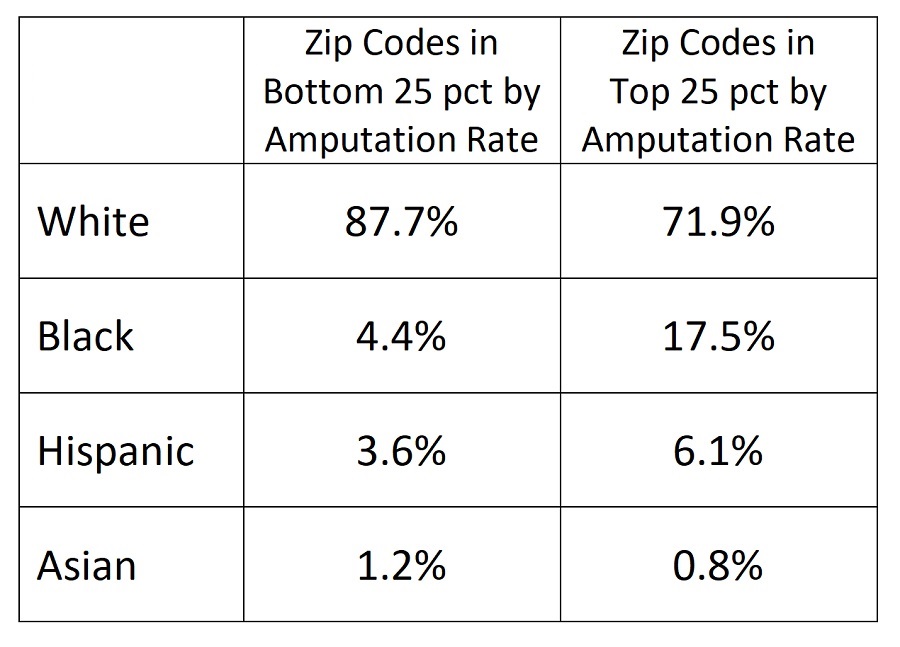
Finally, the data point toward a significant racial disparity in rates of limb loss related to diabetes and PAD. Zip codes with high amputation rates have significantly higher concentrations of Black and Hispanic residents, relative to zip codes with low amputation rates. That conclusion backs up ProPublica’s 2020 investigation about the “epidemic” of limb loss within Black communities. Here are JAHA’s figures:

Significantly, the JAHA study found stark racial and economic disparities within small geographic areas. For example, within the Philadelphia metro area, the zip codes with the highest incidence of vascular-related limb loss overlapped with zip codes having low average incomes and high percentages of Black and Hispanic residents. Similar disparities were found in most urban centers, with low-amputation neighborhoods sitting directly adjacent to high-amputation ones.
“There are multiple potential explanations for gaps in quality care,” the study concludes. In rural areas, geographic distance often deters patients from getting access to routine preventive care that might save a limb, and specialists in diabetes or vascular disease simply aren’t available in many rural communities. Within urban areas, the barriers to health care often include inadequate insurance, lack of health education, and fragmented health delivery systems that allow too many cases to slip through the cracks. “[N]early 4 in 5 Americans who underwent major lower extremity amputation lived in metropolitan areas,” the paper notes, which “highlights the importance of developing programs specifically targeted to improving PAD outcomes among individuals living in urban areas with low [socioeconomic status].”
The paper concludes that the largest short-term impact in limb preservation can be made by “developing programs specifically targeted to improving PAD outcomes among individuals living in urban areas with low socioeconomic status.” Health officials “need to identify and test health services interventions targeting the populations and specific barriers in these communities.”